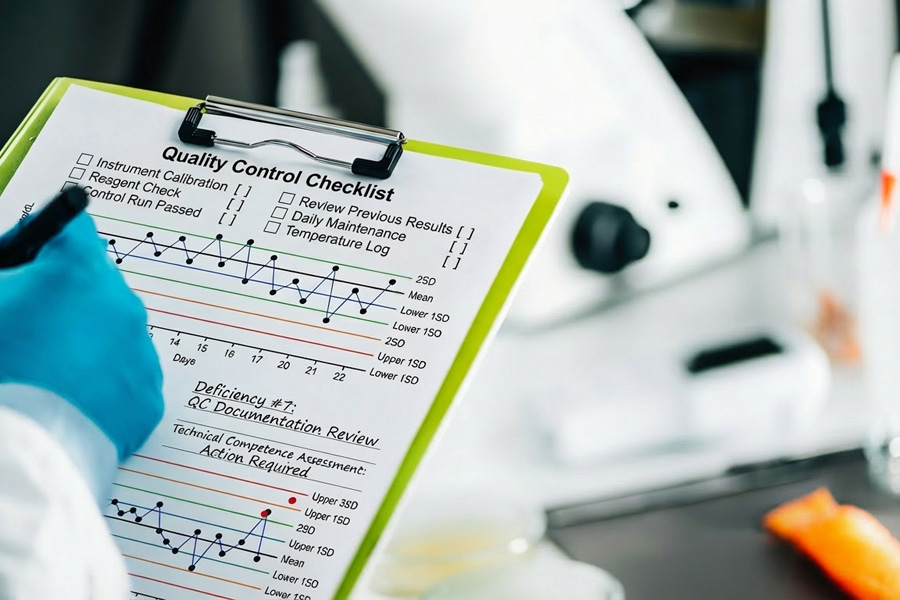
Common COLA and CAP Inspection Deficiencies
January 27, 2026Laboratory Staff Competency Assessment: Meeting CLIA Requirements Year-Round
Why Year-Round Compliance Beats Last-Minute Scrambling
Competency assessment has remained one of the top deficiencies in laboratory inspections for over two decades. CAP data shows it held the number one spot from 2018 through 2020, and it remained in the top four deficiencies through 2022 and 2023 with 644 citations. In 2021, nearly one in five laboratories surveyed by CMS received a competency-related citation.
These numbers tell a clear story: laboratories are still struggling with requirements that have been in place since 1988.
At Laboratory Management Consultants, we see laboratories deal with this struggle all the time. Operating with incomplete documentation, missing assessment windows, or unqualified assessors realizing they have a problem only when a surveyor walks through the door. At that point, what should have been a routine compliance function becomes an expensive emergency.
In this article we walk you through CLIA’s competency assessment requirements, explaining where laboratories often fall short, and showing how to build a year-round program that keeps your lab inspection-ready without the annual scramble.
What CLIA Requires: The Six Elements
CLIA defines laboratory competency assessment as the process by which labs verify that their staff can adequately perform their assigned duties. The regulation applies to all non-waived testing personnel at moderate and high complexity laboratories. Simply training staff is not enough. CLIA requires documentation showing employees performing what they were trained to do, and that demonstration must cover six specific elements.
- Direct observation of routine patient test performance.
The assessor must directly observe the employee handling real patient specimens, including collection (where applicable), processing, and testing. Virtual observation does not satisfy this requirement except where specifically permitted by state law. This element cannot be completed by reviewing records alone. - Monitoring the recording and reporting of test results.
The assessor evaluates how the employee documents and reports results, including the handling of critical values. This includes reviewing how the employee enters results, verifies them, and communicates their findings to the appropriate clinical staff. - Review of intermediate test results, worksheets, QC records, proficiency testing results, and preventive maintenance records.
This element integrates naturally with the monthly supervisory review that most laboratories conduct already. The key is documenting that the review happened and connecting it to a specific employee’s competency record. - Direct observation of instrument maintenance and function checks.
The assessor must observe the employee performing instrument maintenance and calibration verification. This element does not apply to provider-performed microscopy (PPM) procedures, but it does apply to all other non-waived testing systems. - Assessment of test performance through previously analyzed specimens, internal blind testing, or external proficiency testing samples.
Proficiency testing samples can be used for this one, but only after the submission due date has passed. Using PT samples for competency before submission creates a PT handling violation. Alternatively, laboratories can use previously analyzed patient specimens with known results or internally prepared blind samples. - Assessment of problem-solving skills.
This element requires evidence that the employee can identify problems, determine root causes, and take appropriate corrective action. Review of problem logs, QC failure investigations, and corrective action participation all provide documentation for this element.
Timing Requirements: When Assessments Must Be Completed
CLIA sets clear timing requirements that differ based on employee status. New employees must complete semiannual assessments during their first year of testing, meaning two full competency assessments across all applicable test systems before the first year concludes. After the first year, annual assessment is required.
One common misunderstanding involves what “annual” means in practice. CLIA requires evaluations at least annually (typically every 12 months from the previous assessment), not tied to the calendar year.
Laboratories that allow gaps exceeding 18 months between assessments (even when those gaps technically span two calendar years) have received CAP citations. A best practice is to establish a 90-day completion window around each target date, giving staff and assessors a deadline, or a deadline window, in which to get assessments done.
Any time a new instrument or testing methodology is introduced, all affected personnel require new competency assessment before they can report patient results. This is separate from and in addition to their regular annual assessment cycle.
Who Performs Competency Assessments
The qualification requirements for assessors depend on test complexity, and this is an area that catches many laboratories off guard.
- For moderate complexity testing, the Technical Consultant (TC) or individuals meeting TC qualifications must perform assessments.
- For high complexity testing, the Technical Supervisor (TS) is responsible, with the ability to delegate in writing to a qualified General Supervisor (GS).
- For PPM procedures, the Laboratory Director performs assessments, though individual procedures may be delegated in writing.
In December 2024, CMS published a Final Rule that took effect December 28, 2024, harmonizing delegation rules between moderate and high complexity testing. Under the updated rule, moderate complexity assessments can now be delegated to individuals meeting TC qualifications, closing a gap that previously created inconsistency between complexity levels. Laboratories operating under moderate complexity certificates should review their assessor qualification documentation to ensure it reflects this updated standard.
Missing written delegation documentation is a common deficiency. If anyone other than the primary responsible party is performing assessments, that delegation must be documented in writing and retained in personnel files.
Common Deficiency Categories and Why Laboratories Fail
The six required elements have been in place for decades, yet laboratories continue to receive citations in this area. Understanding the most common failure modes helps laboratories build programs to avoid them.
- Incomplete documentation of all six elements. The most common problem is not that laboratories skip assessments entirely, but that they document only a subset of the required elements. Completing five of six elements does not constitute a compliant assessment.
- Timing failures. Missing the semiannual requirement for new employees is a frequent citation. Laboratories sometimes complete an initial orientation assessment and then wait for the annual cycle, leaving a significant compliance gap during the employee’s first year.
- Unqualified assessors. Personnel who do not meet the qualifications for TC, TS, or GS performing assessments creates an immediate deficiency. Written delegation documentation that is incomplete or absent amplifies the problem.
- Failure to assess all test systems. Laboratories sometimes create a single “general competency” assessment rather than system-specific assessments for each test performed. CLIA requires competency assessment for each test system, not a single blanket evaluation.
- Inadequate problem-solving documentation. Element six requires active evidence of critical thinking, not simply a checkbox. Surveyors look for documented examples of the employee identifying problems, investigating root causes, and participating in corrective action.
Building a Year-Round Compliance Program
The most effective approach to competency assessment is also the most practical one: integrate it into processes that already exist in your laboratory. The six required elements map almost entirely onto quality activities that moderate and high complexity laboratories perform routinely.
Monthly supervisory reviews of QC and maintenance records can simultaneously fulfill Element 3 requirements when properly documented as part of an employee’s competency record. Proficiency testing review after submission deadlines covers Element 5. Corrective action documentation already serves Element 6. The task is not creating new processes but connecting existing ones to the competency framework.
Scheduling Best Practices
Assign specific calendar months to each laboratory department rather than managing all assessments simultaneously. Chemistry in January, hematology in February, microbiology in March, and so on. This approach distributes the workload across the year, prevents bottlenecks, and makes it easy to identify when an employee is approaching their assessment window.
For new employees, document the semiannual requirement explicitly in their onboarding record with target completion dates. Many laboratories use 90 days and 9 months as natural checkpoints, which satisfies the semiannual requirement while building in flexibility.
Set calendar reminders 30 days before each assessment window opens. Competency management platforms such as CAP’s Competency Assessment Hub, MediaLab Compass, and StaffReady automate much of this tracking. For laboratories managing assessments manually, a shared spreadsheet with automated conditional formatting achieves similar results at lower cost.
Documentation Standards
Each assessment record should identify the employee by name, list the specific test system, show the assessor’s name and qualification, and include the date. Supporting documentation for each element includes copies of worksheets reviewed, maintenance logs, PT results used, and observation notes. All these should be retained with the assessment record.
When a particular element does not apply to a specific test system, document that fact with an explanation rather than leaving the field blank. A blank field invites a surveyor’s question. A notation reading “No critical values associated with this test system” closes the question before it is asked.
CLIA requires a minimum two-year retention period for competency records, though several states require longer. Verify your state requirements and document your retention policy.
When Competency Assessment Fails: Remediation Protocols
A failed competency assessment does not have to become a personnel crisis if the laboratory has a clear remediation protocol in place. The steps are straightforward, but they must be documented to satisfy regulatory requirements.
When an employee fails an assessment, document the finding immediately and, consistent with your laboratory’s written policy, remove the employee from independent testing in the affected area until competency is demonstrated. Conduct a root cause analysis before proceeding: is the failure due to a gap in the employee’s skills, an unclear procedure, a problem with the assessment tool itself, or a systemic issue affecting multiple staff?
Remediation options progress from least to most intensive based on the root cause. A discussion clarifying misunderstood steps addresses simple knowledge gaps. Reviewing the SOP with the employee and having them observe a competent colleague performing the procedure addresses procedural uncertainty. Practice with known specimens bridges the gap between understanding and execution. Formal retraining is reserved for situations where the above steps do not resolve the deficiency.
Reassessment must follow all remediation and must be documented as a separate event from the original failed assessment. If remediation is unsuccessful after good-faith efforts, permanent reassignment to duties that do not require the failed competency may be necessary. Corrective action should be completed within 30 days of the original finding whenever possible.
Special Situations Worth Planning For
Transfers between CLIA numbers: An employee moving to a laboratory operating under a different CLIA number is treated as a new employee regardless of their experience or the similarity of equipment and procedures. Two semiannual assessments are required in the first year.
Returning employees: An employee who has not performed testing under your laboratory’s CLIA number for more than one year should be treated as a new employee and complete two semiannual assessments in their first year back. Process and equipment changes during their absence make this both a regulatory and a practical necessity.
Cross-trained generalists: An employee who works in multiple departments requires a complete competency assessment for every department where they perform testing. Staggering these assessments across different months prevents the logistical burden from concentrating in a single assessment window.
New instruments: Every staff member who will use a new instrument for patient testing must complete competency assessment before reporting results. This is true even when the instrument replaces a similar platform and the procedures are largely unchanged.
How Laboratory Management Consultants Supports Competency Compliance
Building a compliant, sustainable competency program requires time, expertise, and consistent execution. Many laboratories have the right intentions but lack the structured framework to make it happen year after year.
Laboratory Management Consultants works with physician office laboratories, pain management clinics, and startup diagnostic facilities to develop competency programs that integrate with existing workflows rather than adding to them. Our services in this area include:
- Competency program development. We build custom checklists for each test system, scheduling templates that distribute assessments across the calendar year, and documentation systems that capture all six required elements with appropriate supporting records.
- Training program creation. We develop written training policies and SOPs aligned with competency requirements, ensuring that training and competency assessment work together as a connected system rather than parallel processes that never meet.
- Mock surveys. We conduct personnel file reviews and competency documentation audits that mirror what a CAP, COLA, or CMS surveyor will examine. Identifying gaps before an inspection gives you time to correct them rather than defending them.
- Part-time Laboratory Director services. Our part-time directors provide qualified oversight of competency programs, review and sign off on assessments as required, and maintain the regulatory knowledge base that keeps your program current as requirements evolve.
- Ongoing compliance monitoring. We track regulatory changes from CMS, CAP, and COLA and alert clients to updates affecting their programs. The December 2024 Final Rule changes to delegation requirements are an example of exactly the kind of update that can quietly create a compliance gap if you’re not watching for it.
Competency assessment is one of the most consistently cited deficiencies in laboratory inspections, but it is also one of the most preventable. The requirements are well-defined. The tools to meet them are available. The challenge is building the program infrastructure that makes compliance routine rather than reactive.
Take the Next Step
If your laboratory is approaching an inspection cycle, has recently received a competency-related citation, or simply wants to build a stronger foundation for year-round compliance, we’re ready to help.
Contact Laboratory Management Consultants today at (606) 487-0523 or email tpace@emaillmc.com for a free consultation.
Don’t let a preventable deficiency put your accreditation at risk. With the right program in place, competency assessment becomes a strength rather than a liability.







Medica EasyRA
Thermo Fisher Indiko Plus
Abbott ImmTox 270
The 3200 QTRAP system

The Pictus 500